Spain
Latest News
A cluster of Andes hantavirus infections linked to the Dutch-flagged cruise ship MV Hondius in the South Atlantic has resulted in multiple cases among passengers and crew from several countries. The outbreak involves Andes virus (ANDV), the only hantavirus known to cause limited person-to-person transmission, typically through close and prolonged contact.
Updates on new reported cases between 8 and 15 May 2026:
New cases - three new cases after the after evacuation from the cruise ship:
- One confirmed case in France – who became symptomatic during repatriation.
- One confirmed case in Spain.
- One of the passengers who was evacuated from the ship had a positive result for hantavirus by PCR on 12 May 2026. The person was asymptomatic at the time of testing but successively developed respiratory symptoms. The individual currently remains in isolation.
- One inconclusive case was reported in the United States involving an asymptomatic passenger repatriated on 10 May, with conflicting laboratory results (one positive and one negative from separate laboratories). A second US citizen reportedly developed mild symptoms during evacuation, although details remain unclear based on currently available information.
Total cases:
- 11 cases (8 confirmed, 2 probable, 1 inconclusive case), including 3 deaths.
Other news:
- The cruise ship MV Hondius arrived at the port of Granadilla, Tenerife on Sunday 10 May.
- Disembarkation of guests and part of the crew was carried out and completed on 11 May. Disembarked guests and crew members were transported to the airport and repatriated via evacuation flights throughout 10 and 11 May.
- Evacuation was carried out from Tenerife to the following countries: Spain (14), France (5), Canada (4), the Netherlands (26), UK (22), Ireland (2), Turkey (3), US (17).
- The ship departed Tenerife on 11 May and is expected to arrive in the Netherlands on 17–18 May.
- Preliminary genome sequencing analysis showed high genetic similarities between isolates of Andes virus, likely indicating an initial zoonotic spillover event followed by human-to-human transmission.
- Investigations into the travel history and potential exposures of the first case in the Southern Cone are ongoing and suggest possible exposure to rodents during bird watching activities.
- For details, see ECDC and WHO reports, or on BEACON.
- For contact management: see WHO LINK.
Additional cases among cruise ship passengers remain possible due to the long incubation period of hantavirus infection, which can last up to 6–8 weeks. However, current response measures — including quarantine of disembarked passengers, rapid isolation of suspected cases, and contact monitoring — are expected to reduce the risk of further transmission.
Hantaviruses are rodent-borne zoonotic viruses transmitted to humans primarily through contact with contaminated rodent urine, droppings, or saliva. Human infections are rare but can cause severe and sometimes fatal disease.
Two main clinical syndromes are associated with hantavirus infection:
- Hantavirus cardiopulmonary syndrome (HCPS) occurs mainly in the Americas; it can rapidly progress from fever and flu-like symptoms to respiratory failure, pulmonary oedema, shock, and death. Case fatality is high, typically ranging from 20–40% and may reach up to 50%, particularly among older adults and people with comorbidities.
- Hemorrhagic fever with renal syndrome (HFRS) occurs mainly in Europe and Asia. It primarily affects the kidneys and blood vessels, potentially causing hypotension, bleeding disorders, and renal failure. Case fatality is generally lower, ranging from less than 1% to 15%, depending on the virus and setting.
Transmission: Most hantaviruses are associated with specific rodent reservoir species that carry the virus without apparent illness. Human-to-human transmission is not typically and has only been documented with Andes virus in South America, primarily among close and prolonged contacts. Exposure risk increases during activities that disturb rodent-contaminated environments, such as cleaning enclosed spaces, farming, forestry work, or sleeping in rodent-infested dwellings.
Symptoms usually begin 1–8 weeks after exposure and include fever, headache, myalgia, abdominal pain, nausea, and vomiting.
Diagnosis can be difficult in the early stages because symptoms overlap with influenza, COVID-19, leptospirosis, dengue, viral pneumonia, and sepsis Confirmation relies on serology, especially IgM or rising IgG titres, and RT-PCR during acute illness.
Treatment: There is no licensed specific antiviral treatment or vaccine. Management is supportive, with close monitoring and treatment of respiratory, cardiac, and renal complications. Early recognition and access to intensive care when needed are essential to improve survival.
The risk to the general population is considered very low, while the risk for cruise ship passengers is assessed as moderate. Of note: Even if transmission from evacuated passengers occurs, widespread community spread is unlikely, as Andes virus (ANDV) does not transmit easily and infection prevention measures are in place.
Travel in areas where hanta virus is: Very low risk for travellers.
- Avoid contact with rodents and their feces (wear a mask and gloves when handling a dead/sick animal or cleaning contaminated surfaces). When camping/ecotourism, close tents and cabins to prevent rodents from entering and protect your food from contamination in airtight boxes.
As of March 2026, mpox transmission continues globally across all clades, with clade Ib now confirmed for the first time in Argentina, Ecuador, Austria, the Central African Republic, Russia and Singapore and community transmission documented in five European countries (Austria, Belgium, Portugal, Spain, and the UK).
Sustained community transmission in Madagascar (clade Ib), Pakistan.
DRC Ministry of Health officially declares the end of the mpox epidemic as a national public health emergency on April 2, 2026.
A recombinant clade Ib/IIb strain has been detected in two travelers, with evidence suggesting wider circulation than currently documented (see WHO).
End of March, EMA’s committee for human medicines has issued a recommendation that Tecovirimat SIGA should not longer be used for the treatment of mpox (see EMA).
See also WHO global trends.
Risk very low for general populations but moderate for at risk groups.
Follow recommendations issued by local health authorities.
- Avoid close, skin-to-skin contact with individuals who have, or may have, mpox, including anyone with a rash (pimples, blisters, scabs).
- Wash hands frequently with soap and water or use an alcohol-based hand sanitizer at least 60% alcohol).
- Avoid touching potentially contaminated personal items such as bedding, clothing, towels, cups, or eating utensils used by someone with suspected or confirmed mpox.
- Avoid sexual contact with sick people; use condoms for up to 12 weeks if your sexual partner has had mpox.
- For people belonging to an at-risk group, vaccination may be indicated. See Mpox factsheet. Avoid contact with animals in areas where mpox regularly occurs.
- Avoid eating or preparing meat from wild animals (bushmeat) or using products (creams, lotions, powders) derived from wild animals.
Since the beginning of 2025, and as of 20 August 2025, nine countries in Europe have reported human cases of West Nile virus infection: Albania, Bulgaria, France, Greece, Hungary, Italy, Romania, Serbia and Spain. Currently, 67 areas are known to be affected.
For updates, see ECDC LINK.
The following precautions are recommended:
- Protect yourself against mosquito bites during the day and at night (see optimal mosquito and tick bite protection 24/7).
- Do not touch sick or dead birds, as they may also be infected.
If you have visited a West Nile fever transmission area, do not donate blood for at least 28 days after returning.
Germany: On 3 July 2025, German public health authorities reported detections of circulating vaccine-derived poliovirus type 2 (cVDPV2) in wastewater samples from multiple federal states:
- Dresden (weeks 17, 19, 21, 23)
- Mainz (weeks 15, 19)
- Munich (weeks 21, 22, 23)
- Stuttgart (week 21)
Genetic sequencing shows the viruses closely match the cVDPV2 cluster previously detected in early 2025 in Spain, Poland, Germany, Finland, and the UK.
As of 3 July 2025, no clinical cases of poliomyelitis have been reported in the EU/EEA, and sustained human-to-human transmission within Germany has not been confirmed.
The large geographical spread in the EU/EEA, the fact that detections occurred over several months, and the identification of specific genetic sub-clusters suggest at least some degree of local transmission.
For all individuals, including refugees and migrants: Routine vaccination against polio according to national guidelines is important (Swiss FOPH recommendations | STIKO, Germany recommendations).
Travellers going to countries where wild poliovirus or polio vaccine virus is endemic should get vaccinated against polio, see recommendations on the country pages at www.healthytravel.ch.
On 06 Jun 2025, Spain reported a fatal case of human rabies in a 44-year-old male resident of the Valencian Community.
The patient had been bitten on the right leg by a dog during a trip to Ethiopia in July 2024. He cleaned the wound but did not seek medical attention or receive post-exposure prophylaxis (PEP). Approximately ten months later, he developed nonspecific symptoms, including fever, nausea, and mood changes. These progressed to hydrophobia, leading to a clinical suspicion of rabies. Despite intensive care, he died on 06 Jun 2025.
Spain, including its peninsular territory and islands, has been officially free of terrestrial rabies since 1978, with the exception of an isolated case in June 2013 involving a dog imported from Morocco. However, sporadic imported cases of rabies continue to be reported in the Autonomous Cities of Ceuta and Melilla, primarily involving dogs (four rabies dogs between April to June 2025) and occasionally horses.
This tragic case underscores the importance of awareness about rabies and the critical need for post- exposure prophylaxis following potential exposures, such as dog bites, in rabies-endemic travel destinations, see also rabies factsheet.
Prevention: Avoid contact with animals and do not feed them! Travelers are advised to get a pre-exposure vaccination, especially those at higher risk, such as individuals working with animals, riding two-wheelers, visiting remote areas, young children, cave explorers, or anyone who may come into contact with bats.
Behavior after exposure: After an animal bite/scratch: immediately wash the wound with water and soap for 15 minutes, then disinfect and in any case visit a high-quality medical center for post-exposure vaccination as soon as possible!
Several countries in the European Union have observed an increase in reported cases of hepatis A genotype 1B. In particular, Austria, Czechia and Hungary have observed more reported cases than expected between November 2024 to May 2025.
The increase of HAV infection is mainly affecting adults that are experiencing homeless, people with a drug addiction and people living in poor sanitary conditions. Two genetically closely related clusters of HAV 1b have been identified (cluster a and cluster b).
The chain of transmission is ongoing, and new cases are likely to occur.
Vaccination against hepatitis A is recommended for people visiting friends and relatives in remote rural areas and/or where hygiene conditions are poor as well as for risk persons, see SOP hepatitis A at www.healthytravel.ch PRO version.
Die Daten zu Masernfällen in der Europäischen Union und im Europäischen Wirtschaftsraum (EU/EWR) in den letzten zwölf Monaten (1. Februar 2024 bis 31. Januar 2025 32‘265 Masernfälle) zeigen einen deutlichen Anstieg der Meldungen im Vergleich zu 2023. Rumänien (27‘568), Italien (1‘097), Deutschland (637), Belgien (551) und Österreich (542) wiesen die höchsten Fallzahlen auf.
Aufgrund der vermehrten Viruszirkulation, werden die Fallzahlen sehr wahrscheinlich im Frühjahr 2025 zunehmen. Die anhaltende Übertragung deutet auf Lücken in der Durchimpfung gegen diese vermeidbare Krankheit hin – sowohl bei Kindern als auch bei Jugendlichen und Erwachsenen.
Lassen Sie Ihren Impfstatus überprüfen!
Alle nach 1963 geborenen Personen, die keinen nachgewiesenen Schutz gegen Masern haben (Antikörper oder 2 nachgewiesene Impfungen), sollten zweimal mit dem MMR-Impfstoff geimpft werden. Im Falle einer Epidemie in der Region oder bei Kontakt mit einem Masernfall wird die Impfung ab einem Alter von 6 Monaten empfohlen.
The data from the latest ECDC annual epidemiologic reports on sexual transmitted diseases (STIs) show the notification rate for confirmed gonorrhea cases in European Union/European Economic Area countries rose by 31% in 2023 compared with 2022 and has risen by 321% since 2014.
Syphilis cases also continue to rise. In 2023, 41’051 confirmed cases were reported in 29 EU/EEA countries, representing a 13% increase compared to 2022, and a doubling compared to 2014.
In the past 3 months, vaccine-derived poliovirus type 2 (VDPV2) was detected in sewage samples in Barcelona, Spain; Warsaw, Poland; and Bonn, Düsseldorf, Dresden, Hamburg, Cologne, Mainz and Munich, Germany. The detected virus is genetically linked to a strain that emerged in Nigeria. This strain is circulating in several countries outside the Region, most widely in North and West Africa.
In all 3 countries in the European Region, the virus was isolated from environmental (sewage) samples only – no associated paralytic cases of polio have been detected.
Germany, Poland and Spain maintain strong disease surveillance and high levels of routine immunization coverage, estimated at 85–93% nationally with 3 doses of inactivated polio vaccine (IPV), which provides excellent protection from paralysis caused by poliovirus.
However, pockets of undervaccination exist in every country.
The detection of VDPV2 in wastewater is not surprising. People can shed the virus if they come from or have travelled to countries where oral poliovirus vaccine is still used. The risk for vaccinated people in Germany is very low due to the high vaccination coverage against polio.
For all individuals, including refugees and migrants: routine vaccination against polio according to national guidelines is important (Swiss FOPH recommendations |STIKO, Germany recommendations). Travellers going to countries where wild poliovirus or polio vaccine virus is endemic should get vaccinated against polio, see recommendations on the country pages at www.healthytravel.ch.
In 2024 and as of 2 October 2024, 18 countries in Europe have reported 1’202 locally acquired human cases of West Nile Virus (WNV) infection with known place of infection. The earliest and latest date of onset were respectively on 1 March 2024 and 26 September 2024.
Locally acquired cases were reported by Italy (422), Greece (202), Spain (114), Albania (102), Hungary (101), Romania (71), Serbia (53), Austria (34), Türkiye (30), France (27), Croatia (20), Germany (8), Slovenia (5), Kosovo (4), Slovakia (4), Bulgaria (2), North Macedonia (2) and Czechia (1).
In Europe, 88 deaths were reported by Greece (31), Italy (16), Albania (13), Romania (10), Spain (10), Bulgaria (2), Serbia (2), Türkiye (2), France (1) and North Macedonia (1).
Case numbers reported this year are above the mean monthly case count for the past 10 years. During the same period in 2023, 681 cases had been reported. However, numbers are lower than in 2018, when 1 728 cases had been reported by this time of year.
Distribution of locally acquired human West Nile virus infections in 2024 till 2 October 2024:
Of note, further regions of infection were reported in 2023.
The following precautions are recommended:
- Protect yourself against mosquito bites during the day and at night (see factsheet mosquito and tick bite protection).
- Do not touch sick or dead birds, as they may also be infected.
- If you have visited a West Nile fever transmission area, do not donate blood for at least 28 days after returning.
Crimean-Congo hemorrhagic fever (CCHF) is caused by infection with a tick-borne virus. The disease is prevalent in Eastern Europe, particularly in the former Soviet Union, throughout the Mediterranean region, northwest China, Central Asia, southern Europe, Africa, the Middle East, and the Indian subcontinent.
In the beginning of May 2022, one case of monkeypox was detected in England, which had occurred after travel to Nigeria. In the course of this, 6 further cases of monkeypox were diagnosed in England in people with no previous travel and no contact with known travel-associated cases. These are two cases in one family and four cases in men who have sex with men (MSM). The latter apparently got infected in London. Apart from the family and two of the MSM cases, there are no known links between the cases. Further 2 cases have been reported in the meantime. Investigations into the sources of infection and other suspected cases are in progress.
Additional cases are reported by GeoSentinel and various media reports from the following countries:
- France: 1 suspected case (Île-de-France region).
- Italy: 3 cases, one confirmed, 1 case with travel history Canary Islands (link)
- Canary Islands: 1 suspected case
- Portugal: 14 confirmed cases, another 6 suspected cases (link), Lisbon Region and Tagus Valley Region
- Spain: 7 confirmed, 23 suspected cases, (link)
- Sweden: 1 confirmed case, 1 suspected case
- Canada: 17 suspected cases (link)
- USA: 1 confirmed case with travel history to Canada (link)
Description: Monkeypox is a zoonosis caused by an orthopoxvirus, a DNA virus genetically related to the variola and vaccinia viruses. Monkeypox is endemic in West and Central Africa. Increased cases have been recorded in Nigeria since September 2017, and imports by returning travellers to England and the USA have also been recorded more frequently in recent years. There are two types of monkeypox virus: the West African type and the Central African type (Congo Basin).
Transmission: Monkeypox is transmitted from infected animals by a bite or by direct contact with blood, body fluids or lesions of the infected animal. It can be transmitted via abrasions in the mouth to people who eat infected animals. It can also be transmitted from person to person via the respiratory tract, through direct contact with body fluids of an infected person or with virus-contaminated objects. The incubation period is 5-21 days, usually about 7 to 17 days.
Symptoms: Symptoms of monkeypox include fever, headache, muscle aches, swollen lymph nodes and chills. 1- 3 days after the onset of symptoms, a rash develops that may look like chickenpox or syphilis and spreads from the face to other parts of the body, including the genitals. The disease is usually mild. In immunocompromised individuals, the disease can be severe. The mortality rate is about 1% for the West African type and up to 10% for the Central African type.
For further details, see WHO factsheet, ECDC and CDC.
Further cases must be expected. Persons showing symptoms as described above should contact a doctor, ideally in advance by telephone. Persons who have several sexual partners or practice casual sex should be particularly vigilant!
Prevention: Good personal hygiene, avoid contact with infected persons and animals at all costs. During stays in West and Central Africa: No consumption of bushmeat. The individual risk of contact with a patient with monkeypox depends on the type and duration of contact. In the case of very close contact with a case (e.g. family members, aeroplane neighbours, medical personnel), the risk of infection has so far been classified as moderate; in the case of sexual / intimate contact, it is probably high.
Source image: NCDC
WHO 18.5.2022, RKI 19.5.2022, UK GOV, 16.5.2022, Outbreak News Today, 18.5.2022, CDC, Labor Spiez
General Information
Vaccinations for all travellers
All travellers should have completed a basic immunisation according to the Swiss vaccination schedule, LINK.
In cases of incomplete or unknown immunization status, catch-up vaccinations are strongly recommended, and individuals should be followed up until the vaccination series is completed (note: environmental samples have tested positive for cVDPV2).
- Polio is a vaccine-preventable viral disease of the nervous system that is acquired mainly through the consumption of food or water contaminated by feces.
- The infection with the poliovirus can affect children and adults and may lead to permanent limb or respiratory muscle paralysis and death.
- An effective, well-tolerated vaccine is available! Check if booster doses are recommended (on top of completed basic vaccination schedule).
EKRM_Factsheet_Layperson_EN_Polio.pdf
- Polio is a vaccine-preventable viral disease of the nervous system that is acquired mainly through the consumption of food or water contaminated by feces.
- The infection with the polio virus can affect children and adults and may lead to permanent limb or respiratory muscle paralysis and death.
- An effective, well- tolerated vaccine is available! Check if booster doses are recommended for the travel destination (on top of completed basic vaccination schedule).
Regular hand washing after using the bathroom and before eating or preparing food. Avoidance of undercooked or raw food that is potentially contaminated with fecal material.
The most important prevention is vaccination. A very effective and well-tolerated vaccine against polio is available (inactivated (killed) polio vaccine (IPV)), which is part of the basic vaccination schedule during childhood. Combination vaccines (e.g. with diphtheria and tetanus) are also available. After basic vaccination, a booster dose is recommended every 10 years for travel to certain countries (see country page recommendations). WHO recommends a yearly vaccination for residents or long-stay visitors (minimum 4 weeks) in a country with ongoing polio infections or circulating vaccine-derived polio viruses. This recommendation not only targets individual protection, but aims to prevent the international spread of the virus.
All travellers should have completed a basic immunisation and boosters according to the Swiss vaccination schedule, LINK.
All travellers should have completed a basic immunisation and boosters according to the Swiss vaccination schedule, LINK.
General information on measles, mumps and rubella (MMR)
Please consult the following FOPH links:
Travellers should be immune to chickenpox. Persons between 13 months and 39 years of age who have not had chickenpox and who have not received 2 doses of chickenpox vaccine should receive a booster vaccination (2 doses with minimum interval of 4 weeks), see Swiss vaccination schedule, LINK.
Please consult the following link of the FOPH:
General information about chickenpox (varicella) and shingles (herpes zoster)
Vaccinations for some travellers
- Hepatitis B is a liver infection caused by a virus.
- The virus is transmitted through sexual contact, but can also be transmitted through blood (products), e.g. when sharing syringes, tattoo needles, etc.
- There is a safe and very effective vaccine that offers long-lasting protection.
- The hepatitis B vaccination is recommended for all infants and adolescents up to the age of 16 and for risk groups regardless of age.
- Hepatitis B is a liver infection caused by a virus.
- The virus is transmitted through sexual contact, but can also be transmitted through blood (products), e.g. when sharing syringes, tattoo needles, etc.
- There is a safe and very effective vaccine that offers long-lasting protection.
- The hepatitis B vaccination is recommended for all infants and adolescents up to the age of 16 and for risk groups regardless of age.
- Federal Office of Public Health (FOPH). Hepatitis B:
https://www.bag.admin.ch/bag/en/home/krankheiten/krankheiten-im-ueberblick/hepatitis-b.html - Hepatitis Switzerland: https://en.hepatitis-schweiz.ch/all-about-hepatitis/hepatitis-b/
- There is a risk of rabies in the African territories of Ceuta and Melila in Spain.
- Rabies has not been reported in domestic or wild animals in the rest of Spain (including the Balearic Islands and Canary Islands). However, bats may carry bat lyssavirus (bat rabies).
- Rabies is mainly transmitted by dogs (and bats), but any mammal can be infectious.
- The disease is invariably fatal at the time when symptoms occur.
- Rabies is best prevented by a pre-travel vaccination and appropriate behavior towards mammals (avoiding contacts).
- Pre-travel vaccination (see section prevention) is also recommended because vaccines and immunoglobulins are often not available in many travel countries.
- Attention: a bite or a scratch wound as well as a contact with mammal saliva on an open wound is always an emergency! Find out about the necessary actions below!
- Rabies is mainly transmitted by dogs (and bats), but any mammal can be infectious.
- The disease is invariably fatal at the time when symptoms occur.
- Rabies is best prevented by a pre-travel vaccination and appropriate behavior towards mammals (avoiding contacts).
- Pre-travel vaccination (see section prevention) is also recommended because vaccines and immunoglobulins are often not available in many travel countries.
- Attention: a bite or a scratch wound as well as a contact with mammal saliva on an open wound is always an emergency! Find out about the necessary actions below!
(range: 4 days - several years!) and manifests itself as encephalitis (inflammation of the brain), which in 99.99% of cases is fatal within a few weeks. As soon as symptoms of encephalitis appear, a fatal course can no longer be prevented.
No treatment against rabies disease exists!
Post-exposure measures: clean the wound immediately with plenty of water and soap for 10-15 minutes, then disinfect the wound (e.g. Betadine®, Merfen®), and immediately (i.e. during the trip!) get emergency post-exposure vaccination against rabies: for those having received full pre-exposure rabies vaccination before travel, two additional vaccine shots (any available brand) at an interval of 3 days suffice and should be administered as soon as possible on site (i.e. also while travelling). If full pre-exposure vaccination has not been given, in addition to vaccination, passive immunization is required with immunoglobulins within the shortest delay on site.
Of note, immunoglobins (and sometimes vaccines) are often unavailable in low-resource settings, causing stress and uncertainty. Tetanus booster vaccination may be also warranted.
Petting any mammals while travelling is not a good idea, even if they are cute! Do not feed them! Refrain from touching wild or unfamiliar or dead animals.
Vaccination against rabies (preexposure vaccination) is recommended for most travellers, and is particulary recommended for:
- Repeated travels or long-term stay in endemic countries.
- Short journeys with high individual risk, especially for travellers on ‘two wheels’ or treks in remote areas, toddlers and children.
- Persons, working with animals, or cave explorers (bats!).
The shortened vaccination schedule can be proposed to most travellers: 2 doses given at least 7 days apart before departure. A single lifetime booster dose (3rd dose) is recommended after one year or later when further travelling to rabies endemic countries is undertaken. If you have an immune deficiency, please consult your doctor, as different vaccination intervals apply to you.
- In case of trips planned, schedule a visit at the travel clinic 4 weeks before departure at the latest. But if it's really urgent, an appointment 10 days before departure will suffice.
- After exposure (bite, scratch injury): seek medical attention immediately (meaning even during travel!) to get wound treatment and postexposure vaccinations against rabies! This is also necessary even for those with a completed series of basic vaccinations before travel!
- This information leaflet should be printed and kept handy during the trip!
- FOPH Switzerland: LINK
- Chikungunya fever is a viral infection that is transmitted by mosquitoes.
- The disease typically manifests itself with fever and severe joint pain in the hands and feet, which can last for weeks to months in some patients.
- Chikungunya fever can be prevented by protecting yourself from mosquito bites.
Chikungunya_Factsheet_Public_ECTM_EN.pdf
Insect_and_Tick_Bite_Protection_Factsheet_Public_ECTM_EN.pdf
Map, see publication: Chikungunya virus: epidemiology, replication, disease mechanisms, and prospective intervention strategies, JCI, 2017, LINK.
- Chikungunya fever is a viral infection that is transmitted by mosquitoes.
- The disease typically manifests itself with fever and severe joint pain in the hands and feet, which can last for weeks to months in some patients.
- Chikungunya fever can be prevented by protecting yourself from mosquito bites.
The infection may cause some or all of the following symptoms: sudden onset of high fever, headache, muscle and joint pain, joint swelling, rash. The rash usually appears after the onset of the fever and usually affects the trunk and extremities. The joint pain and swelling usually occur symmetrically on both sides and mainly affect the hands and feet - but larger joints such as the knees or shoulders can also be affected. The intense joint pain can be very debilitating for those affected.
Around 5 - 10 % of those infected have persistent severe joint and limb pain even after the fever has subsided, which in some cases lasts for several months or, although rarely, even years.
Preventive measures against mosquito bites during the day: Apply mosquito repellent to uncovered skin; wear long clothing; treat clothing with insecticide. For more information, see the information sheet "Protection against insect and tick bites". Another very important protective factor is so-called 'environmental hygiene': breeding sites for mosquitoes in the immediate vicinity of human dwellings should be avoided by removing all forms of containers with water (e.g. flowerpot saucers, uncovered water containers, etc.).
Vaccination: A chikungunya vaccine (VIMKUNYA®) is licensed in Switzerland. The Swiss Expert Committee on Travel Medicine has issued a vaccination recommendation for travellers, see LINK.
- Only a few tick species bite and spread pathogens that cause disease in humans.
- The diseases transmitted in an area depend on the local tick species.
- Ticks live in grassy, brushy, or wooded areas and on animals.
- Outdoor activities like walking your dog, camping, gardening, or hunting increase risk off exposure—even in your own yard.
- Get vaccinated against tick-borne encephalitis (TBE) if in an affected area.
- Only a few tick species bite and spread pathogens that cause disease in humans.
- The diseases transmitted in an area depend on the local tick species.
- Ticks live in grassy, brushy, or wooded areas and on animals.
- Outdoor activities like walking your dog, camping, gardening, or hunting increase risk off exposure—even in your own yard.
- Get vaccinated against tick-borne encephalitis (TBE) if in an affected area.
Depending on the geographical region and the species, ticks may carry and transmit different pathogens. Diseases include the human ehrlichiosis, Lyme disease, tularemia, babesiosis, tick-borne relapsing fever, Rocky Mountain spotted fever, other rickettsioses, some arboviral diseases, and several flaviviruses causing encephalitis such as tick-borne encephalitis (TBE). Some ticks may also cause tick paralysis.
In Europe, commonly transmitted disease by ticks include Lyme disease (borreliosis), tick-borne encephalitis and tularemia.
In the US (and less so in South America) important tick-borne diseases represent babesiosis, anaplasmosis and ehrlichiosis, Powassan disease and severe fever with thrombocytopenia syndrome (STFS).
Other important pathogens transmitted by ticks are bacterial organisms causing rickettsial diseases, which are found throughout the world. Among returned travelers, rickettsial diseases have been estimated to be the fourth most common cause of fever, with symptoms such as rash, abdominal pain, and a dry, black/dark scab at the site of the infecting bite.
Tick-borne diseases may occur worldwide, but distribution is based on geographical location (see map).
Areas with increased risk of TBE include central and eastern Europe and the Baltic and Nordic countries. TBE is also prevalent in Russia all the way from the western border with Europe to its eastern border.
Lyme borreliosis is the most prevalent tick-transmitted infection in temperate areas of Europe, North America and Asia, and its geographic distribution is ever-increasing. Central Europe is the region with the highest tick infection rates (young ticks/nymphs >10%; adult ticks >20%) in Europe, specifically in Austria, Czech Republic, southern Germany, Switzerland, Slovakia and Slovenia.
Babesiosis is found in certain regions of North America and forested areas in Europe and East Asia. Anaplasmosis is common in North America, Europe, and China.
Ehrlichiosis is common in the US, certain areas of Europe, South America, and Africa.
Powassan disease is found in the northeastern US and far eastern Russia, whereas Severe Fever with Thrombocytopenia Syndrome (SFTS) occurs in the US and Asia-Pacific region.
Rickettsial infections are present worldwide. African Tickbite Fever (ATBF) is the most commonly reported rickettsial infection acquired during travel and occurs in southern Africa (especially Botswana, South Africa, and Zimbabwe).Mediterranean Spotted Fever (MSF), reported among returning US and UK travelers, occurs over much of Africa, Europe, India, and the Middle East; whereas Rocky Mountain Spotted Fever (RMSF) is commonly found throughout Canada, parts of Central and South America, and the US.
Crimean-Congo hemorrhagic Fever (CCHF) is a rare but serious viral disease transmitted by tick bites or contact with infected animal blood. It is the most widespread viral hemorrhagic fever, found in Eastern and Southern Europe, the Mediterranean, northwestern China, central Asia, Africa, the Middle East, and the Indian subcontinent. Healthcare workers and those handling livestock face higher risk.
The key to prevent tick-borne diseases is to protect yourself from tick bites (see also fact-sheet "Mosquito and tick bite prevention"):
- Use insect repellent
- Wear long-sleeved shirts, pants and socks
- Treat clothing and gear with 0.5% permethrin
- Perform thorough tick checks after spending time outdoors. Important: with some pathogens, attachment time of the tick is key for successful disease transmission, and quick riddance may therefore prevent infection.
The best prevention against tick-borne encephalitis (TBE) is to get vaccinated; this is recommended if living or travelling in an endemic area. The vaccine protects against all virus subtypes.
- In risk areas, make sure you have good tick protection: Wear skin-covering clothing and closed shoes and use repellents.
- After spending time in risk areas: check your body for ticks remove them immediately, and disinfect the bite.
- Monitor the bite site and see a doctor if symptoms appear. For post-travel symptoms, consult a tropical medicine specialist.
- Vaccination against TBE is recommended for all residents of an endemic areas and for travelers visiting such areas, especially those engaging in outdoor activities.
- Covid-19 is a disease that affects the whole body, but mainly shows with respiratory symptoms such as cough and difficulty in breathing. It is caused by the SARS-CoV-2 virus.
- The infection is mainly spread through respiratory droplets and possibly aerosols when infected persons cough, sneeze, speak or sing without wearing a mask.
- The infection can be prevented very effectively by vaccination and an increasing number of vaccines are now approved and available for protection.
- Vaccination is recommended according to the Swiss recommendations of the Federal Office of Public Health (FOPH), see LINK.
- Furthermore, prevention relies heavily on people wearing face masks, on hand hygiene and on physical distancing (min. 1.5 m) if masks are not worn and people are not vaccinated.
- Influenza is common all over the world including sub-tropical and tropical countries.
- Vaccination offers the best protection.
- Vaccination against flu is recommended for all travellers who belong to an “at risk” group such as pregnant travellers, travellers with comorbidities, elderly people (>65 years), or who plan a a high-risk trip (e.g. cruise-ship, pilgrimage).
- The influenza vaccine does not offer protection against avian flu.
General informations about seasonal flu (influenza)
Please consult the following FOPH links:
Other health risks
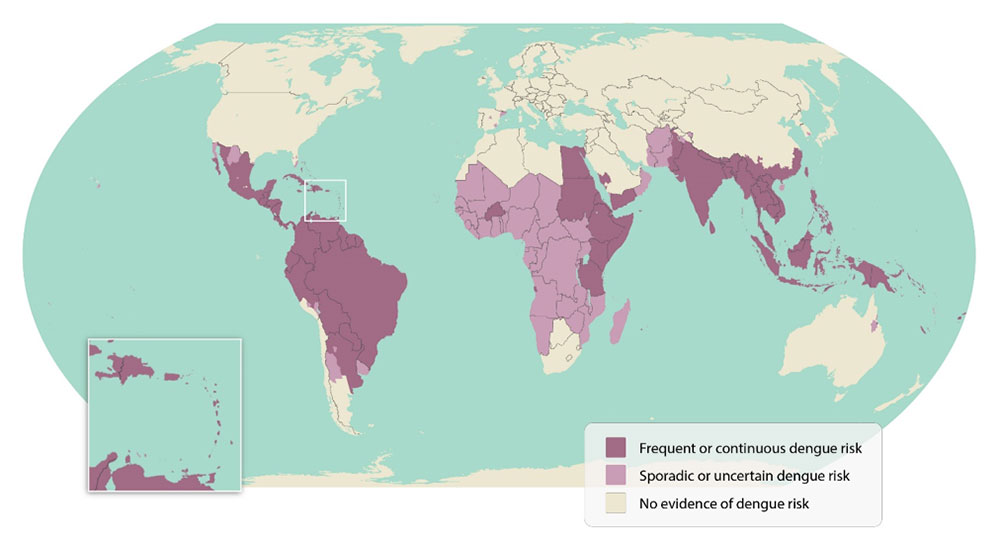
During 2018 the first locally acquired dengue cases were reported, with transmission occurring in the provinces of Cádiz, Catalonia and Murcia. Risk is low.
- Dengue fever is the world's most common insect-borne infectious disease.
- Great attention should be paid to mosquito protection (day-biting mosquito)!
- The disease can cause high fever, muscle and joint pain, and skin rash. In rare cases, bleeding may occur.
- There is no specific treatment. Vaccination is recommended only for persons with evidence of previous dengue infection.
- For personal safety, we strongly recommend that you inform yourself in detail about dengue.
Dengue_Factsheet_Public_ECTM_EN.pdf
Insect_and_Tick_Bite_Protection_Factsheet_Public_ECTM_EN.pdf
- Dengue fever is the world's most common insect-borne infectious disease.
- Great attention should be paid to mosquito protection (day-biting mosquito)!
- The disease can cause high fever, muscle and joint pain, and skin rash. In rare cases, bleeding may occur.
- There is no specific treatment. Vaccination is recommended only for persons with evidence of previous dengue infection.
- For personal safety, we strongly recommend that you inform yourself in detail about dengue.
{kind=link}
In 3 out of 4 cases, an infection with the virus remains asymptomatic. After a short incubation period (5-8 days), 1 out of 4 infected people present an abrupt onset of fever, headache, joint, limb and muscle pain, as well as nausea and vomiting. Painful eye movement is also typical. A rash may appear on the 3rd or 4th day of illness. After 4 to 7 days, the fever subsides but fatigue may persist for several days or weeks.
In rare cases, severe dengue can occur. Particularly susceptible are local children and seniors, as well as people who have experienced a prior dengue infection. Tourists very rarely present with severe dengue. In the first days, severe disease resembles the course of classic dengue fever, then on the 4th/5th day, and usually after the fever has subsided, the condition worsens. Blood pressure drops, and patients complain of shortness of breath, abdominal discomfort, nosebleeds, and mild skin or mucosal hemorrhages. In the most severe cases, life-threatening shock may occur.
There is no specific treatment for dengue virus infection. Treatment is limited to mitigation and monitoring of symptoms: fever reduction, relief of eye, back, muscle and joint pain, and monitoring of blood clotting and blood volume. Patients with severe symptoms must be hospitalized.
For the reduction of fever or pain, remedies with the active ingredient paracetamol or acetaminophen are recommended (e.g. Acetalgin® Dafalgan®). Drugs containing the active ingredient acetylsalicylic acid (e.g. Aspirin®, Alcacyl®, Aspégic®) must be avoided.
Effective mosquito protection during the day and especially during twilight hours (i.e. sunset) is the best preventive measure:
- Clothing: Wear well-covering, long-sleeved clothing and long trousers, and treat clothing with insecticide beforehand.
- Mosquito repellent: Apply a mosquito repellent to uncovered skin several times a day.
- Environmental hygiene: Do not leave containers with standing water (coasters for flower pots, etc.) in your environment to avoid mosquito breeding sites.
For further information, please refer to the factsheet on "Mosquito and tick bite protection".
Note on the dengue vaccine Qdenga®:
- Based on the data available, many European countries, as well as the Swiss Expert Committee for Travel Medicine (ECTM), currently recommend vaccination with Qdenga® only for travelers who have evidence of a previous dengue infection and who will be exposed in a region with significant dengue transmission, for details see LINK. A consultation with a specialist in tropical and travel medicine is recommended.
- About 1 in 4 vaccinated persons experience malaise and fever for a few days about 1-2 weeks after vaccination.
Consistent mosquito protection during the day (see above) is still considered the most important preventive measure against dengue!
- Do not take any products containing the active ingredient acetylsalicylic acid (e.g. Aspirin®, Alcacyl®, Aspégic®) if you have symptoms, as they increase the risk of bleeding in the event of a dengue infection!
- However, do not stop taking medications containing acetylsalicylic acid if it is already part of your regular treatment for an underlying condition.
- Vaccination against Dengue fever for travellers – Statement of the Swiss Expert Committee for Travel Medicine, an organ of the Swiss Society for Tropical and Travel Medicine, July 2024, LINK.
- Dengue Map (Center for Disease Control and Prevention – CDC): https://www.cdc.gov/dengue/images/areaswithrisk/Dengue-World-Map.jpg
- Tigermücke, SwissTPH
- www.tiger-platform.eu
There is a risk of arthropod-borne diseases other than malaria, dengue, chikungunya or zika in sub-/tropical regions, and some areas of Southern Europe. These include the following diseases [and their vectors]:
- in Europe
- Borreliosis, FSME (= tick-borne encephalitis), rickettsiosis [ticks]
- Leishmaniasis [sand flies]
- West-Nile fever [mosquitoes]
- in Africa
- Rickettsiosis, in particular African tick bite fever [ticks]
- Leishmaniasis [sand flies]
- African trypanosomiasis = sleeping sickness [tsetse flies]
- West-Nile fever [mosquitoes]
- in Asia
- Scrub typhus [mites]
- Rickettsiosis [fleas or ticks]
- Leishmaniasis [sand flies]
- West-Nile fever [mosquitoes]
- Crimea-Congo-hemorrhagic fever [ticks]
- in North and Latin America
- Rickettsioses and in particular Rocky Mountain spotted fever [ticks]
- Leishmaniasis and Carrion's disease [sand flies]
- American trypanosomiasis = Chagas disease [triatomine bugs]
- West Nile fever [mosquitoes]
- Sexuell übertragbare (oder transmissible) Infektionen (STI) sind eine Gruppe von viralen, bakteriellen und parasitären Infektionen; während viele behandelbar sind, können einige zu Komplikationen, schweren Erkrankungen oder zu einer chronischen Infektion führen.
- STI nehmen weltweit zu.
- Lesen Sie das folgende Informationsblatt für weitere Informationen.
- Geschlechtskrankheiten sind ein weltweit verbreitetes Gesundheitsproblem und können durch Prävention, regelmässiges Testen und Behandlung in den Griff bekommen werden.
- Das Wissen um Risiken sowie Safer-Sex-Praktiken inklusive Kondomgebrauch sind wichtig. Falls Sie mehr dazu erfahren wollen, wie Sie sich während der Reise optimal schützen können, besprechen Sie dies mit einer Fachperson.
- Hatten Sie eine Risikosituation, ist es wichtig mit einer Fachperson so rasch wie möglich Rücksprache zu halten, um zu erörtern, ob eine HIV-Post-Expositions-Prophylaxe (PEP) durchgeführt werden soll, um eine Ansteckung mit HIV zu verhindern.
- Im Nachgang einer Risikosituation ist es wichtig sich auf Geschlechtskrankheiten testen zu lassen. Auch dann, wenn Sie keine Symptome haben.
- Brennen oder Juckreiz im Genitalbereich
- Schmerzhaftes oder häufiges Wasserlösen oder auch Schmerzen im Unterleib
- Ungewöhnlicher Ausfluss aus dem Penis oder der Vagina
- Wunden, Rötungen, Bläschen im Mund/Lippen oder Genitalbereich sowie Warzen im Intimbereich
- Manchmal auch Fieber (eher selten)
Wichtig: Eine STI kann auch ohne oder mit nur leichten Symptomen auftreten. Auch wenn Sie sich dessen nicht bewusst sind, können Sie andere anstecken. Deshalb ist es wichtig sich testen zu lassen.
- Beachten Sie die Safer Sex Regeln von Love Live. Dazu gehört auch bei jedem Anal- oder Vaginalverkehr Kondome zu verwenden.
- Denken Sie daran, dass es bei Oralverkehr auch zu Übertragungen von STIs kommen kann.
- Lassen Sie sich impfen! Es gibt Impfstoffe zum Schutz vor HPV, Hepatitis A und Hepatitis B.
- Hatten Sie eine Risikosituation, ist es wichtig mit einer Fachperson so rasch wie möglich Rücksprache zu halten, um zu erörtern, ob eine HIV-Post-Expositions-Prophylaxe (PEP) durchgeführt werden soll, um eine HIV-Infektion zu verhindern. Am wirksamsten ist eine HIV-PEP innerhalb weniger Stunden danach.
- Es gibt auch weitere Präventionsmassnahmen für spezielle Situationen (Präexpositionsprophylaxe HIV-PrEP). Sprechen Sie mit einer damit erfahrenen Fachperson vor Abreise darüber.
- Denken Sie daran, dass Alkohol oder Drogen zu erhöhtem Risikoverhalten führen.
- Denken Sie daran, dass Sie eine weitere Person/bekannter Partner*in bei ungeschütztem Sex anstecken können, sofern bei Ihnen eine unbehandelte STI vorliegt.
- Menschen mit einer neu diagnostizierten STI sind angehalten ihre früheren Sexualpartner*innen zu informieren, damit auch sie behandelt werden können.
Durch Bakterien oder Parasiten hervorgerufen
Alle diese Krankheiten können geheilt werden. Wichtig ist dabei, frühzeitig zu testen und umgehend zu therapieren, um Komplikationen und v.a. weitere Übertragungen zu vermeiden.
- Syphilis
Auch bekannt als Lues. Sie wird durch das Bakterium Treponema pallidum verursacht. Das erste Anzeichen ist eine schmerzlose Wunde an den Genitalien, im Mund, auf der Haut oder im Rektum, die hochgradig ansteckend ist und nach 3 bis 6 Wochen spontan abklingt. Da diese schmerzlos ist, nehmen nicht alle Patienten*innen diese Läsion wahr. Oft heilt diese Infektion jedoch nicht von selbst aus. In der zweiten Phase können Hautausschlag, Halsschmerzen und Muskelschmerzen auftreten. Unbehandelt kann die Krankheit im Verborgenen (latent) bleiben, ohne dass Symptome auftreten. Etwa ein Drittel der Infizierten mit unbehandelter Syphilis entwickelt im Verlauf Komplikationen. Diese Spätform wird als sogenannt tertiäre Syphilis bezeichnet . In diesem Stadium kann die Krankheit alle Organe befallen: am häufigsten das Gehirn, die Nerven und die Augen. Die Infektion kann während der Schwangerschaft auf den Fötus und bei der Geburt auf das Kind übertragen werden. - Chlamydia trachomatis
Chlamydien können ungewöhnlichen Ausfluss aus dem Penis oder der Vagina, Unbehagen beim Wasserlösen und Unterleibsschmerzen verursachen. Oft treten keine Symptome auf. Unbehandelt können sie zu Unfruchtbarkeit führen und die Krankheit kann auf Sexualpartner*innen übertragen werden. Die Bakterien können auch während der Schwangerschaft auf den Fötus, oder während der Geburt auf das Kind übertragen werden und Augeninfektionen oder Lungenentzündungen verursachen. - Gonorrhoe
Auch bekannt als Tripper. Zu den häufigsten Symptomen gehören Ausfluss aus der Vagina oder dem Penis und schmerzhaftes Wasserlassen. Symptome müssen aber nicht immer auftreten. Sowohl bei Männern als auch bei Frauen kann Gonorrhoe auch den Mund, den Rachen, die Augen und den Anus infizieren und sich auf das Blut und die Gelenke ausbreiten, wo sie in eine schwere Krankheit übergehen kann. Bleibt sie unbehandelt, kann sie eine Beckenentzündung verursachen, die zu chronischen Beckenschmerzen und Unfruchtbarkeit führen kann. Die Krankheit kann während der Schwangerschaft auf den Fötus übertragen werden. - Weitere bakterielle STIs: Mykoplasmen und Ureaplasmen. Diese können ebenfalls behandelt werden.
- Trichomoniasis
Sie wird durch einen Parasiten verursacht, der mit einer einzigen Dosis eines Antibiotikums behandelt werden kann. Trichomoniasis kann bei Frauen einen übel riechenden Scheidenausfluss, Juckreiz im Genitalbereich und schmerzhaftes Wasserlassen verursachen. Bei Männern treten in der Regel weniger oder keine Symptome auf. Zu den Komplikationen gehört das Risiko einer vorzeitigen Entbindung bei schwangeren Frauen. Um eine Reinfektion zu verhindern, sollten beide Sexualpartner behandelt werden.
Durch Viren hervorgerufen
- HIV/AIDS - siehe Informationsblatt HIV-AIDS
- Herpes simplex Virus
Im Lippen-Mundbereich, auch bekannt als Fieberbläschen, ist nicht heilbar. Herpes kann aber mit Medikamenten bei akuten Beschwerden kontrolliert werden. Die Symptome sind in der Regel schmerzhafte, wässrige Hautbläschen und finden sich an oder um die Genitalien, den Anus oder den Mund. Nach der Erstinfektion ruht das Virus im Körper und die Symptome können über Jahre hinweg wieder auftreten. Schwangere Frauen können die Infektion an ihre Neugeborenen weitergeben, was zu einer bedrohlichen Infektion führen kann. - Virale Hepatitis (siehe auch Hepatitis Schweiz)
- Hepatitis A (HAV)
Hepatitis A ist eine durch Impfung vermeidbare Leberinfektion, die durch das Hepatitis-A-Virus verursacht wird. Das Hepatitis-A-Virus findet sich im Stuhl und im Blut infizierter Personen. Hepatitis A kann durch verunreinigtes Wasser und Lebensmittel sowie bei anal-oralen sexuellen Aktivitäten übertragen werden. Die Patienten*innen leiden an einer akuten und oft schweren Erkrankung, erholen sich aber allermeist spontan. - Hepatitis B (HBV)
Das Hepatitis-B-Virus wird durch sexuelle Kontakte sowie durch den Kontakt mit anderen Körperflüssigkeiten, wie z.B. Blut, übertragen. Zur Übertragung kann es z.B. auch bei medizinischen Eingriffen oder Brennen eines Tatoos unter nicht optimalen hygienischen Bedingungen kommen. Hepatitis B kann eine schwere Leberinfektion verursachen, die sowohl zu einer sofortigen Erkrankung, als auch zu einer lebenslang andauernden Infektion führen kann mit möglicher Folge einer dauerhaften Lebervernarbung (Zirrhose) und Krebs. Schwangere Frauen mit Hepatitis B können das Virus während der Geburt auf ihr Kind übertragen. Zu Beginn der Infektion haben Sie möglicherweise keine Symptome. Das Virus kann auf Sexualpartner*innen übertragen werden. Hepatitis B kann mit antiviralen Medikamenten behandelt werden, ist aber nur selten heilbar. Eine Impfung kann eine Hepatitis-B-Infektion verhindern. - Hepatitis C (HCV)
In den meisten Fällen wird Hepatitis C durch den Kontakt mit infiziertem Blut übertragen. Seltener kann es durch analen Sexualkontakt oder von der Mutter auf das Kind während der Schwangerschaft und Geburt übertragen werden. Die meisten Infizierten sind sich ihrer Infektion nicht bewusst, weil sie keine Symptome entwickeln, aber diese chronische Infektion kann zu Leberzirrhose und Krebs führen. Hepatitis C kann behandelt werden, eine Impfung gibt es nicht.
- Hepatitis A (HAV)
- Humanes Papillomavirus (HPV)
HPV ist die häufigste Geschlechtskrankheit. Es gibt eine Vielzahl verschiedener HPV-Typen, und einige von ihnen können Genital-, Anal- und Mundwarzen sowie Gebärmutterhals-, Penis- oder Rachenkrebs verursachen. Die Symptome können auch noch Jahre nach dem Sex mit einer infizierten Person auftreten. Zwei verfügbare Impfstoffe schützen gegen die wichtigsten HPV-Typen, die Gebärmutterhals-, Penis- oder Analkrebs verursachen. - Zika - siehe Informationsblatt Zika
In den meisten Fällen wird es vor allem durch Stechmücken übertragen. Es kann aber auch sexuell übertragen werden. Eine Ansteckung mit Zika während der Schwangerschaft kann bei dem sich entwickelnden Fötus Geburtsfehler wie Mikrozephalie (kleiner Kopf mit neurologischen Ausfällen) verursachen. Die einzige Möglichkeit, eine sexuelle Übertragung des Virus während der Schwangerschaft zu verhindern, besteht darin, Vorsichtsmassnahmen (Kondome) zu treffen oder Sex (mindestens 2 Monate nach der Rückkehr) mit jemandem zu vermeiden, der kürzlich in ein Risikogebiet gereist ist, auch wenn der Reisende keine Symptome hat.
- Love Life: www.lovelife.ch
- Sexuelle Gesundheit Schweiz: www.sexuelle-gesundheit.ch
- Hepatitis Schweiz: https://hepatitis-schweiz.ch/formen/was-ist-hepatitis
- World Health Organization (WHO). Factsheets. Sexually transmitted infections (STIs). 14 June 2019: www.who.int/news-room/fact-sheets/detail/sexually-transmitted-infections-(stis)
- Centers for Disease Control and Prevention (CDC). Factsheet: Information for Teens and Young Adults: Staying Healthy and Preventing STDs (2017): www.cdc.gov/std/life-stages-populations/stdfact-teens.htm
- Centers for Disease Control and Prevention (CDC). How You Can Prevent Sexually Transmitted Diseases: www.cdc.gov/std/prevention/
- Centers for Disease Control and Prevention (CDC) Sexual Transmission and Prevention. Zika Virus: www.cdc.gov/zika/prevention/protect-yourself-during-sex.html
- Centers for Disease Control and Prevention (CDC) Zika and Pregnancy; Pregnant Women and Zika (March 2021): www.cdc.gov/pregnancy/zika/protect-yourself.html
- Altitude sickness can be life-threatening and may be experienced by any traveler.
- The danger begins at around 2500m and rises with increasing altitude.
- People differ in their susceptibility to altitude sickness; this is not related to their physical fitness.
- Severe altitude sickness with fluid accumulation in the brain or lungs can rapidly result in death.
- If you are planning a stay in high altitudes, we strongly recommend you to consult your doctor for detailed recommendations and instructions.
- Eine Höhenkrankheit kann lebensgefährlich sein und bei jedem Reisenden auftreten.
- Die Gefahr beginnt bei ca. 2500m und nimmt mit zunehmender Höhe zu.
- Wenn Sie einen Höhenaufenthalt planen, lesen sie bitte dieses Merkblatt aufmerksam durch!
- Je nach Reiseart und / oder Vorerkrankungen wird die Beratung durch eine Fachperson dringend angeraten.
- Langsamer Aufstieg. Aufstiegsregeln: oberhalb von 2500m sollte die Schlafhöhe um nicht mehr als 300-500m pro Tag gesteigert werden und pro 1000m Schlafhöhengewinn sollte ein zusätzlicher Ruhetag eingelegt werden.
- Treten Beschwerden auf, die auf eine Bergkrankheit hinweisen (siehe oben), muss der Anstieg pausiert werden und er darf erst wieder bei Beschwerdefreiheit fortgesetzt werden. Bei Zunahme der Beschwerden muss abgestiegen werden bzw. Patient:innen in tiefere Lagen abtransportiert werden. Bei Ignorieren zunehmender Beschwerden können sich die lebensbedrohlichen Formen der Höhenkrankheit, das Höhenhirnödem und/oder das Höhenlungenödem entwickeln.
- Ist das Einhalten der oben genannten Aufstiegsregeln situativ oder geländebedingt nicht möglich, kann die Einnahme von Acetazolamid (DIAMOX®) das Risiko eine akute Höhenkrankheit zu entwickeln, vermindern. Die Verschreibung des Medikaments bedingt eine ärztliche Indikationsstellung sowie eine Aufklärung über allfällige Nebenwirkungen!
- Kopfschmerzen: Paracetamol (z.B. PANADOL®, DAFALGAN®). Keine Schlafmittel verwenden!
- Höhenhirnödem: sofortiger Abstieg. Falls verfügbar: Sauerstoffgabe, medikamentöse Notfalltherapie.
- Höhenlungenödem (Atemnot auch in Ruhe, rasselndes Atemgeräusch, Reizhusten) Sofortiger Abstieg. Falls verfügbar: Sauerstoffgabe, medikamentöse Notfalltherapie.
- Mpox is a viral disease that typically causes a rash, swollen lymph nodes and fever.
- An emerging variant is spreading rapidly in eastern D.R. Congo and neighbouring countries, leading the WHO to declare a new Public Health Emergency International (PHEIC) in August 2024.
- Close physical contact (sexual or non-sexual) is the main route of transmission.
- The disease is usually mild. Children, pregnant women and people with weakened immune systems are most at risk of complications.
- Take general precautions (see factsheet) to prevent the disease.
- There is a vaccination against Mpox, but it is currently only available for people at high risk.
- Mpox is a viral disease that typically causes a rash, swollen lymph nodes and fever.
- An emerging variant is spreading rapidly in eastern D.R. Congo and neighboring countries prompting a new WHO declaration of a public health emergency of international concern (PHEIC), as of August 14th 2024.
- Close physical contact (sexual or non-sexual) is the main mode of transmission.
- The disease generally follows a mild course. Children, pregnant women, and people with weak immune systems are the most at risk of complications.
- Vaccination against mpox is available, but limited to groups at high risk of exposure.
Mpox has been commonly found in West and Central Africa for many years where the suspected reservoir - small mammals - is endemic. There are two types of Monkeypox virus called ‘clades’ that cause the disease mpox - clade I in Central Africa and clade II in West Africa. Since the end of smallpox vaccination campaigns in the early 1980’s, cases of mpox have increased, slowly at first and significantly in the last 5-10 years, especially in the Democratic Republic of Congo (DRC).
In 2022, a new emerging subclade of clade II was responsible for a global epidemic that spread mainly through sexual contact among men who have sex with men. It resulted in the first public health emergency of international concern (PHEIC) declared by the WHO until 2023. Although the clade II epidemic is now under control, this virus variant continues to circulate worldwide.
In 2024, the continued spread of mpox clade I in endemic regions of Central Africa, particularly in the DRC, and the emergence of a new subclade Ib in Eastern DRC and neighboring countries have raised global concern and prompted the WHO to declare a PHEIC for the second time in two years. The current geographical spread of the mpox clade Ib variant occurs via commercial routes through sexual contact (e.g. sex workers), followed by local transmission in households and other settings (which is becoming increasingly important).
Animal to human transmission
Mpox can spread from animal to human when they come into direct contact with an infected animal (rodents or primates).
Human to human transmission
Mpox can be spread from person to person through close physical contact (sexual and non-sexual contact) with someone who has symptoms of mpox. Skin and mucous membrane lesions, body fluids, and scabs are particularly infectious. A person can also become infected by touching or handling clothing, bedding, towels, or objects such as eating utensils/dishes that have been contaminated by contact with a person with symptoms. Household members, family caretakers, and sexual partners of a confirmed case of mpox are at higher risk for infection as are health care workers who treat a case without adequate personal protection.
The incubation period (time between infection and onset of symptoms) ranges from a few days up to 3 weeks. Mpox causes a rash / skin eruption that can be painful associated with swollen lymph nodes and fever. Fever may start already before the rash phase. Other symptoms include muscle aches, back pain, and fatigue. The rash may be localized or generalized, with few or hundreds of skin lesions. It mainly affects the face, the trunk and the palms of hand and soles of the feet. It can also be present in genital areas and on mucous membranes such as in the mouth and throat. Symptoms usually last 2 to 4 weeks and the person remains contagious until all lesions have healed (once the cabs have fallen off).
Complications include secondary bacterial infections, infections of the lung and brain and involvement of other organs, still birth and others. Children, pregnant women, and people with weak immune systems are at higher risk to develop a severe form of mpox.
The majority of person with mpox recovers spontaneously and do not need specific antiviral treatment. Care management consists of relieving pain and other symptoms and preventing complications (e.g., superinfection). Several antiviral treatments are studied in various countries and may be used in trials or in clinical situations according to the recommendations of national medical societies.
In case of symptoms:
- Seek medical attention immediately
- If you are diagnosed with mpox
- Please stay at home (isolate yourself) until your mpox rash has healed and a new layer of skin has formed. Staying away from other people and not sharing things you have touched with others will help prevent the spread of mpox. People with mpox should regularly clean and disinfect the spaces they use to limit household contamination.
- Wash your hands often with soap and water or an alcohol-based hand sanitiser containing at least 60% alcohol.
- You should not have sex while symptomatic and while you have lesions or symptoms. Use condoms for 12 weeks after infection. This is a precaution to reduce the risk of spreading the virus to a partner.
- For more information on what do if you are sick, see CDC LINK.
General precautions:
- Worldwide:
- avoid close, skin-to-skin contact with people who have or may have mpox or people who have a rash (e.g., pimples, blisters, scabs).
- Wash your hands often with soap and water or an alcohol-based hand sanitiser containing at least 60% alcohol.
- Avoid touching potentially contaminated personal items such as cups, bedding/clothing, towels or sharing eating utensils/cups, food or drink with a person who has, or may have mpox.
- Avoid sex with sick persons; use of condoms for up to 12 weeks if you sexual partner have had mpox.
- Follow advice of local authorities.
- When travelling to endemic / epidemic areas in Africa, in addition to above mentioned general precautions:
- Avoid contact with and animals in areas where mpox regularly occurs.
- Avoid eating or preparing meat from wild animals (bushmeat) or using products (creams, lotions, powders) derived from wild animals.
Vaccination:
There are several vaccines against mpox (e.g. Jynneos®, manufacture Bavarian Nordic). The Bavarian Nordic vaccine was originally developed to fight against smallpox, but offers a cross-protection against mpox. In Switzerland, the Jynneos® vaccine has been licensed by Swissmedic since 2024. Groups at risk (e.g., men who have sex with men or transgender people with multiple sex partners) are eligible for vaccination since 2022 and this recommendation remains unchanged (see FOPH recommendations). In light of the epidemiological situation in Africa in 2024, the Swiss Expert Committee for Travel Medicine recommends vaccination against mpox for professionals who are / will be in contact with suspect mpox patients or animals in endemic/epidemic regions or who work in a laboratory with the virus (for updates, see news).
The risk to the general population and travelers (tourists) is considered extremely low if the above-mentioned general precautions are followed and vaccination is not recommended.
- Seek medical attention immediately.
- Mpox is not a sexual transmitted disease in the strict sense, physical contact with a person with symptoms of mpox (rash at any stage) is sufficient to transmit the disease. Condoms do not protect you from getting mpox!
- There are other important travel related health risks such as diarrhoea, road traffic accidents, air pollution and more.
- For more information, see the section "Healthy Travelling".